Supporting oncology professionals through education
The content on this site is intended for healthcare professionals only
The content on this site is intended for healthcare professionals only
Elysse Bautista Gonzalez1, Andrés Quintero Leyra2, Teresa Verenice Munoz Rocha3, Heber Tomás Reyes-García4, Enrique Soto-Perez-de-Celis5, Alejandra Palafox1, Alejandro Mohar Betancourt6,7, Richard Sullivan8
Fundación Mexicana para la salud (FUNSALUD), Tlalpan, Ciudad de México, México
Public Health Department, Faculty of Medicine, National Autonomous University of Mexico. Ciudad de México, México
Centro de Investigación en Nutrición y Salud, Instituto Nacional de Salud Pública, Santa María Ahuacatitlán, Cuernavaca, Mor, 62100, México
Centro Médico Nacional 20 de Noviembre, Benito Juárez, Ciudad de México, México
Division of Medical Oncology, University of Colorado Anschutz Medical Campus, Aurora, CO, USA
National Cancer Institute of Mexico, Mexico
National Autonomous University of Mexico, Mexico
Institute of Cancer Policy, Centre for Cancer, Society and Public Health, King’s College, London, UK
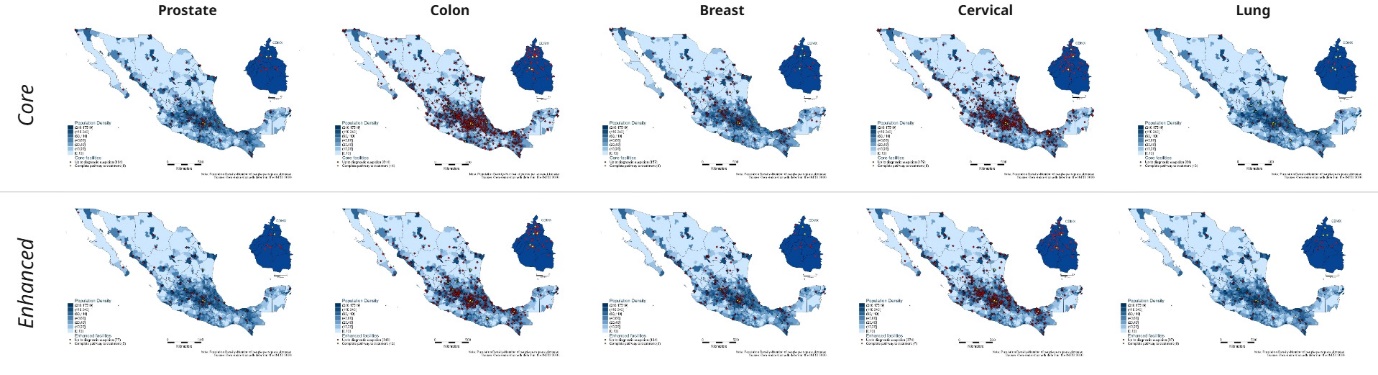
Comprehensive assessments of infrastructure and human are needed to understand the cancer delivery service gaps. This study seeks to map oncological infrastructure of the Ministry of Health in Mexico for five types of cancer: breast, lung, prostate, colon, and cervix.
Through a realist evaluation of publicly available databases from the High Specialty Medical Equipment National Inventory and the General Direction of Health Information, a comprehensive identification and classification of cancer resources was conducted with the intended outcome to map cancer care infrastructure in Mexico. Guided by the literature, resources necessary for diagnosis and treatment were selected by an expert consensus. Thereafter, facilities were classified by service scope into either diagnostic or diagnostic and therapeutic, and by infrastructure level into core or enhanced. Results were then mapped against municipal population density(1).
From N = 14,133 unique healthcare facilities that deliver any type of healthcare, only 5% provided cancer care. Enhanced cancer care options are less common than core services (N=686 vs N=404) and most facilities focus on diagnostic services rather than full treatment. Additionally, our results show the healthcare facilities available for cancer types are unequal and not necessarily aligned with the epidemiological burden; they are also centralised in the country and not aligned with population density(1).
In the maps below, population density is marked in blue. For both core and enhanced infrastructure maps, red facilities are those available for each cancer type only for diagnosis; those marked in yellow are available for treatment(1).
Policy recommendations include: 1) Increase the number of facilities capable of undertaking full diagnosis and treatment and enhanced care, 2) Equitable allocation of resources in densely populated areas, 3) Regional and national decentralisation of available infrastructure and 4) Allocation of equitable infrastructure per cancer type.
Bautista-Gonzalez E, Quintero Leyra A, Munoz Rocha TV, Reyes-García HT, Soto-Perez-de-Celis E, Palafox Parrilla A, Mohar Betancourt A, Sullivan R. Assessing disparities in cancer resources distribution in Mexico. BMC Health Serv Res. 2025 Apr 17;25(1):564.
We are an independent charity and are not backed by a large company or society. We raise every penny ourselves to improve the standards of cancer care through education. You can help us continue our work to address inequalities in cancer care by making a donation.
Any donation, however small, contributes directly towards the costs of creating and sharing free oncology education.
Together we can get better outcomes for patients by tackling global inequalities in access to the results of cancer research.
Thank you for your support.