ASCO 2024
Pfizer RT
Prof Martin Schostak – University Hospital Magdeburg, Magdeburg, Germany
Dr Alexander Wyatt – Vancouver Prostate Centre, Vancouver, Canada
Prof Charles Ryan – University of Minnesota, Alexandria, USA
Dr Emmanuel Antonarakis – University of Minnesota, Minnesota, USA
MS: Hello and welcome. My name is Martin Schostak, I’m a urologist from Magdeburg in Germany. So my first question is to Dr Wyatt, to explain to us what, from your point of view, are the most important points concerning the functional aspects of HRR testing?
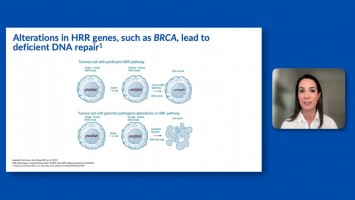
AW: I think it’s important to remember that in the metastatic state something like a quarter of all patients can have some sort of defect in a gene that’s linked to DNA damage repair. Now, functionally those can actually have quite different effects. So we know that BRCA2 mutations and homozygous solutions can lead to homologous recombination repair deficiency and exquisite sensitivity to a PARP inhibitor in that context. We also know that there are rare alterations in other HRR-related genes that can also lead to bona fide homologous recombination repair deficiency. But there are other genes, such as ATM, CDK12 and some others that are linked to DNA damage repair in general but may not lead to an HRD phenotype in testing.
MS: So that’s very important but what we read during the last years from different societies and different recommendations when and how to test and if we should do in every case a molecular tumour board or not. So we have very different opinions about this, so I’m very curious what do we think about early or late testing Dr Antonarakis? What is your point?
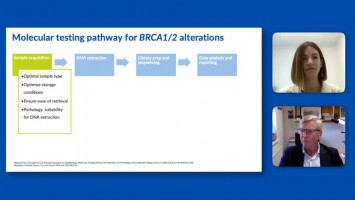
EA: Let’s begin with some background, just to set the stage, where genetic testing or genomic testing encompasses many different things. For our patients it means two different things – one is the inherited genes that they were born with which we call the germline mutations or the germline DNA. This is important, not just to the patient’s treatment or prognosis but also for their family considerations. They might have first degree relatives that need to be tested if they have a positive germline inherited, a BRCA2 mutation for example. The second, which is quite different, is the tumour testing itself which is sometimes called somatic DNA repair mutations. So here we’re talking about mutations that can arise in the cancer after the person was born during the course of their life and there may have been a trigger – it could have been environmental, just bad luck. But the key thing there is that those mutations are not inherited, they did not come from a parent and they cannot be passed to the subsequent generation. Oftentimes when a patient hears, ‘You have a BRCA2 mutation,’ we need to be very clear with that patient what’s the origin of that mutation – did this comes from an inherited gene that was derived from one of the parents or was this just found in the tumour and it’s not inherited. The only way they can tease those two apart is to do both types of tests in every patient. So how is this done? Germline DNA can be done usually from a saliva sample or blood sample, some other ways to do it. Remember, we do not need tumour tissue for that because that’s just the genes present in every single cell in your body, including the cancer cell but also every other cell. Then the somatic testing we do need a tumour sample. This can be an archival biopsy, it can be, for example, the prostate biopsy, prostatectomy, or it can be a metastatic biopsy. In recent years we could even get tumour DNA mutations from the circulations – circulating tumour DNA. So there are many ways to test; we should be very clear with our patients that both are required for all patients with metastatic disease. That’s the part that we all agree with. Both with family counselling and with patients and for therapeutic implications.
MS: Coming back to the testing you said your point on the search for somatic mutations and germline mutations. So when a patient comes to us normally he knows perhaps in his family there are some relatives having cancer but all these mutations are not easy to understand. So what is easier to go first, for genetic testing, for germline testing or to go first for the disease, for patient’s opinion/point of view, and to do somatic testing? What is more important?
CR: So I think to answer your question is that the more we can learn about the tumour in the patient, the better over time. Of course family testing is important once we’ve identified a mutation but genetic testing, next generation sequencing, on tumours now tells us so much more than whether or not there’s a BRCA2 mutation. It tells us about TP53 status and RB and it tells us about other potential mutations that may be present. So I think our role as oncologists and those who are treating advanced prostate cancer is to try to integrate the biology of the disease we’re treating with our treatment choices and our counselling of the patient and their potential outcomes. So the short answer to your question is I think somatic testing is the most important and then I would reflex to doing family testing if I see a mutation that I think… a BRCA2 mutation, for example, that one would propose is likely to be in the family. Then that’s very important also.
MS: We know that best would be a marker that’s predictive, so question for Dr Wyatt. But if we do such next generation sequencing coming from tissue or from circulating DNA or whatever, how sure is that genetic material?
AW: I totally agree with Chuck that panel testing, NG testing, is getting more and more comprehensive. We’re getting more and more information about a person’s cancer and I think that can only be helpful, looking to the future. But many of the things that we identify are probably primarily prognostic in nature, so something like a TP53 mutation would be quite prognostic. We do know for DNA, selected DNA damage repair defects, and BRCA2 is kind of at the vanguard of that, that there is predictive relevance for vulnerability to certain types of therapy such as the PARP inhibition. Now, they do also, however, carry prognostic weight as well. So we know that men with germline BRCA2 mutations are more likely to be diagnosed with advanced disease, may have more rapid progression on other standard of care treatments. The same appears to be true of somatic alterations in, say, CDK12. So most of the mutations that we identify have prognostic weight but it’s really exciting that some of them are predictive biomarkers for PARP inhibition response.
MS: So if we think on testing, what’s the best moment? When we have a first diagnosis of, let’s say, locally advanced prostate cancer, some lymph node metastases we know that it will observe rapid progression. Do we test this patient or should we wait and on the moment of metastatic castration resistant prostate cancer or is it for second or third line? When is the best moment to test?
EA: Yes, let’s talk about something obvious which is that germline DNA does not change over time. So there is no reason not to test germline DNA after the very first encounter if that patient has not done it before. That’s the easy one, I want to get that out of the way, and it has family implications and also therapeutic implications. So that we should do for every patient with at least intermediate to high-risk localised disease, locally advanced disease and metastatic disease. Then the other aspect becomes a little bit more nuanced and that is when do we get somatic testing. I don’t think a patient with localised curable prostate cancer needs to undergo somatic testing. Why? Number one, the chance to cure it with conventional surgical or radiotherapeutic approaches is high and so there’s no reason to think about a targeted systemic therapy for that patient. And none of them are approved by the EMA or FDA in that context anyway. In the metastatic disease it becomes a little bit more complicated. Metastatic hormone sensitive patients will all over time, or at least a vast majority, develop castration resistant disease in the future. So one way to think about it is you’re getting a test now to plan for that next step. Many of us in this room are ordering these tests for metastatic patients even at the time when they are still hormone sensitive. We’re doing it with whatever biopsy is available. By the way, one of the nice things about HRR genes and their mutations is that in most cases, there are a few exceptions, but in most cases a mutation is truncal. What that means in real life is the mutation is either there or not there when the cancer develops and it usually does not become acquired over time and it’s usually not a mutation that is acquired in the castration resistant state if it’s not there in the hormone sensitive state. That’s not true at all of TP53 mutations or RB1 inactivation or androgen receptor mutations which clearly accumulate over time and might be present in the CRPC state even though they are not present in the HSPC state. Because of that interesting fact, it’s worthwhile, in my opinion at least, testing the HRR gene mutations from a biopsy, because the absence of that mutation usually means that it’s not going to be acquired over time and the presence of that mutation that is there in the beginning, in the primary tumour clone will likely be there in most, if not all, of the metastatic tumour clones including the CRPC clones.
MS: We know that, especially with BRCA mutations, of very early mutations in cancer - the same for all the other panel of mutations? Or what do you think? Is there possibility that the mutation comes later or is it always present when the cancer develops?
CR: It’s not always present when the cancer develops, they can occur as acquired somatic alterations, that has been shown in studies that have been done with serial cell-free DNA testing in patients as their disease develops over time. The aspirational interpretation of your question is that over time we hope to be serially sampling the tumour through liquid mechanisms and be able to respond to that evolving biology. Now, we can see the evolving biology but we don’t really have many drugs that are actionable against these alterations that occur. But we do when it comes to PARP inhibitors. So, for example, in the case where a somatic alteration may not be present it can occur over time and that would indicate an emerging indication for a PARP inhibitor. Dr Wyatt may be able to answer better than I can how frequent those types of acquired alterations are because they’re not common but they do occur.
AW: I think the vast majority of BRCA2 and other DNA damage repair defects are there very early in disease. But I think they can be missed even if they are present in primary tissue because we may not have caught the dominant foci on a biopsy. So there is some added value but, of course, it’s not as high as for RB1 or androgen receptor. One key thing to remember is one of the reasons that we all agree that testing early is important in a man with metastatic disease is also that the turnaround time for testing can be long. Sometimes even just retrieving a tissue block can take a while, the testing process can then take a while and then you may still actually have a fail at the end. So at least if you have a long runway for the test there, then you have the opportunity to reflex to other modalities – germline testing or ctDNA testing – at progression. Whereas if you leave this until the CRPC setting then you might get a little bit behind.
MS: So what about liquid biopsies?
CR: So in which tissue is it best to test?
MS: Yes, is a liquid biopsy better or…?
CR: It’s a great question. I think that they are complementary in many ways. A liquid biopsy is not going to be effective in the context of controlled disease when the disease burden is low and it’s a really critical point. So if you see a patient with metastatic disease, for example, and then you start them on ADT and another agent and their PSA goes to zero and you think, ‘Now I should check,’ you’re probably going to have a negative result. You’re probably not going to have any circulating tumour DNA; you may have some cell-free DNA but it may be the non-cancerous DNA.
MS: That means liquid biopsy only for patients in progression?
CR: Or initial diagnosis. Yes, when there’s a substantial disease burden is when.
MS: Yes, and archival tissue is always present, you can use that.
CR: Exactly, yes.
MS: It’s a very important point. We have new recommendations coming out, treatments like PARP inhibitors. At least in Germany sometimes choice basically probably depends on what the patient had before and it’s more the opinion than the PARP inhibitor deciding which combination we will take. What do you think about it?
EA: We have some Europeans and some Americans and at least a Canadian on the panel and I think we should go by region of the world. In the United States the combinations of olaparib and abiraterone or enzalutamide plus talazoparib require a gene test, either somatic or germline. The European Medicine Agency, I believe, has approved those without a prior therapy. This is in the first line mCRPC setting in the combination with ARPI. So you might argue that in European countries such as Germany if you have a first line mCRPC patient who has not received an ARPI or a PARP inhibitor you could offer that patient a combination of talazoparib plus enzalutamide or olaparib plus abiraterone. The counter-argument to that is that even though this may be approved in a broader indication in European countries there is still a greater degree of benefit to patients with germline or somatic BRCA2 mutations, maybe BRCA1 or perhaps CDK12 as well. When we are discussing risks or benefits with that patient, so now the context matters and, of course, the clinical is one aspect, but the molecular context is also important for weighing the risks and benefits. I would argue that this does not apply to the US because you cannot use those combinations in an agnostic fashion. But in European countries if I knew that a patient had a BRCA2 mutation then I would discuss olaparib plus abiraterone versus the alternative options such as docetaxel chemotherapy, such as it is an ARPI alone with tissue. When weighing those three or four different options in the context of the BRCA2, steering towards the PARP inhibitor combination. But in the absence of that, and especially in the absence of all HRR mutations, this would be panel testing these days, we’re not just testing one gene, if they’re all negative I would find it more difficult even though I still could prescribe it in Europe, find it more difficult to give a PARP inhibitor combination in that setting as opposed to other life prolonging therapies.
MS: So there’s a kind of clinical in testing if we have efficacy or not. Of course we should think on and its toxicity and….
CR: Cost and toxicity? I think we still struggle a little bit with what’s the mechanism of that interaction in the non-HRR mutated patients whereby those two drugs would work better than one alone. There’s some great pre-clinical science in that area but I don’t think we’ve really definitively discovered what that mechanism is.
MS: Yes, It’s very good. What do you think of the BRCAAway study, does it kind of prove?...
CR: It’s certainly moving us closer. I think it supports this notion that there may be some interaction but I would say we still have a little more to learn on that front.
MS: So we have learned many things about the optimum point of testing and optimum way of testing and early testing is important. We may have prognostic information about potential BRCA-targeted treatment with PARP inhibitors or not and this can help to make the clinical decisions with the patient in the tumour board which treatments would be the next choice. I think we don’t have actually a clear way which is common for all countries. My opinion, we should sit together and have this kind of conference, in between ESMO, ASCO and so on, concerning the molecular tumour board and how to process all these things in clinical reality. This is important. For the moment my opinion is that the testing, especially next generation sequencing, is highly expensive and this means in clinical practice that these are academic decisions to do this, we don’t have all the academic institutions making all the decisions in Germany. So to bring this Information into daily practice for every patient it’s difficult and we should find an easier way to clarify when it’s really helpful and when it’s only academic, and what you said are very important points. Have you seen any very important abstracts at this conference concerning mutations or the methods to discover the mutations, Dr Wyatt?
AW: There were several really exciting emerging approaches that get other ways to detect homologous recombination repair deficiency, beyond looking for mutations in the DNA. So we know if you sequence the entire genome you can see the scars of a BRCA2 defect, for example, without actually finding that BRCA2 defect. So that’s a really promising way to identify the phenotype of homologous recombination repair deficiency. It’s unclear at the moment whether we can do this from targeted sequencing; I would say perhaps there’s reasonable sensitivity but not very good specificity yet from targeted sequencing for phenotyping. But another really promising approach is looking at RAD51 foci and trying to look at from a pathologic standpoint can you see evidence of active damage to the DNA or that HRD phenotype in the tumour tissue. So there’s a nice abstract from Joaquin Mateo’s lab which is really showing proof of principle for doing this from a pathology standing.
MS: Thank you very much. I think such molecular tumour board we are doing actually, but different experts is very important also in daily practice and work together and find some discussion in every situation of the patient together with the family, or with the patient alone is important to help take the decision together with the physicians. I think we are done, actually. Thank you very much for this very wonderful discussion and your points. Thank you also for watching.